
The Nordic Conference on Digital Health and Wireless Solutions (NCDHWS 2026) convened at the University of Oulu’s Kontinkangas campus on 16 and 17 June 2026. The event was hosted by the university’s 6GESS and DigiHealth research programmes and opened by conference president Professor Jarmo Reponen. Invited speakers travelled from across Europe and beyond, from Catalonia to Johns Hopkins, Taiwan and Australia. Across two days, and from very different starting points, speakers kept returning to the same problem. Building a digital health tool is rarely the hard part. The hard part comes later, when it has to win clinicians’ trust and keep working in everyday care.

Opening the conference, Minister of Science and Culture Mari-Leena Talvitie placed the field in a national frame. ”Health and wellbeing are the key growth sectors of the future,” she told the room, and pointed to what she called a historic national investment in research and development.

Building the infrastructure, piece by piece
Joan Guanyabens, Director of the TIC Salut i Social Foundation in Catalonia, opened the conference with a long view. Catalonia runs a tax-funded, universal, multi-provider system with more than a hundred providers. ”We have 10 million people at this moment,” Guanyabens said, and the legacy they are served by is not tidy. ”This is really a huge problem. We have 28 different hospital information systems integrated into a single public network.” Since 1998 the region has built the pieces one by one. A unique patient identifier, electronic prescribing that links doctors, patients and pharmacies, a shared record built across the systems through interoperability, a personal health record that citizens only truly took up during the pandemic, and digital imaging across every hospital, now reaching into pathology and genetics.

Guanyabens was candid that the work is unfinished and, in places, unruly. Even within a single hospital, data from one vendor can be hard to read, and across vendors harder still. His main prescription was interoperability, built in when systems are designed rather than added afterwards, alongside open platforms. ”We have to chase a clinical data repository, and we are migrating all solutions, all data to this clinical data repository,” he said. The plan extends to a marketplace of applications and services, and to a greater say for citizens in how the system is governed.
Catalonia’s approach to artificial intelligence starts from the problem, not the technology. A strategic committee picks a clinical problem it wants solved, from stroke imaging to dermatology to a voice assistant for primary care. The region then buys a certified solution if one exists, or builds one with a university or company if it does not.
Making systems work, and keeping them working
Professor Sabine Koch of Karolinska Institutet argued that a digital health service succeeds or fails on how it is designed and run. It does not fail on the technology itself. Building it is the easy part. Keeping it in use is harder.

Europe has its grand plan, the European Health Data Space, but the daily reality is messier. The staff who enter the data are often not the ones who benefit from it. Systems throw up side effects no one intended. The stress of poorly fitted IT is a known cause of doctor burnout.
Koch’s remedies were unglamorous. Design the service around the people who use it, to a recognised standard, involve real users, fit it to how the workplace actually functions, and keep testing it rather than signing it off once. And do not confuse adoption with success! A service lasts only if it is also affordable, secure, well governed and not wasteful of resources.

Professor Arild Faxvaag of NTNU, a rheumatologist, made the case for learning health systems. ”The health system is my patient,” he said, and diagnosed it much as he would a patient. He plotted care on two axes, how long a problem has been present and how many competences it takes to treat, and concluded that Nordic systems handle simple, acute problems well and chronic, multimorbid ones poorly. On rare and complex diseases his verdict was blunt: ”too few people learn too little, too late.”
Healthcare itself is an information system, Faxvaag argued. So, adding an electronic record means fitting one information system inside another. The effects are slow and not always positive. When changing the system, he described withdrawal effects among clinicians as well as implementation ones, drawn from Epic experience in Norway, Denmark, and Finland —and lags in which a decision taken in year zero shows its effect around year eight. His proposal was to weave the cohort-centred data spaces the Nordics already hold into everyday clinical work, put patients in control of their own data, and treat the natural occurrence of disease as a resource for developing and validating knowledge.
Trust as the test for AI
Professor Karim Lekadir of the University of Barcelona built his talk around a single word —trust — and began from familiar ground. Within months of the first COVID-19 vaccine, millions of people accepted it, because decades of experience tell us how to develop, validate, and regulate a vaccine. A young technology like medical AI carries no such track record. This makes trust harder to earn.
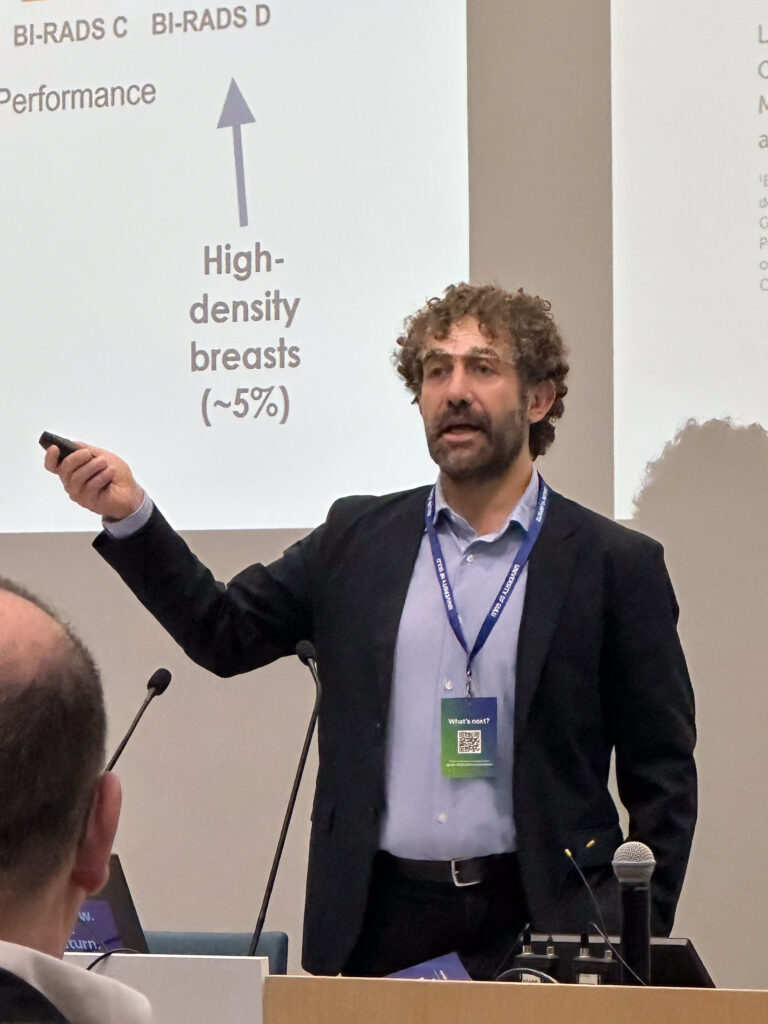
His lead example was an algorithm that caught breast tumours six clinicians had missed, the small and difficult ones in particular. He used it to make the opposite case. The same tool missed obvious tumours, little had been disclosed about how it was built, and it had been validated only in the United Kingdom and the United States. When Lekadir’s group built its own version in Barcelona, the tool proved unfair, performing worse for the roughly 5% of women with high-density breasts. Performance, he argued, is not the same as trustworthiness. His FUTURE-AI framework, built on international consensus, sets six requirements for a clinical tool. It should be fair, universal, traceable, usable, robust, and explainable.
Lekadir also pressed hard on method. The usual way of building medical AI is to define a problem, grab whatever hospital data is available, train a model, and push up its accuracy. That leaves out the people the tool is meant to serve. ”Engage them first,” Lekadir argued, ”and they redefine the task.” Ask cardiologists what a heart-failure tool should predict, and they want to know how the heart is functioning and how the patient is likely to fare, so they can adjust treatment. Ask patients, and they want something else entirely. Not a mortality score, but a warning when fatigue or pain is coming.
A focus group in Peru raised a source of bias his team would not have thought to test. The country has people living at sea level and others high in the Andes, and their physiology differs enough to skew a model trained on one or the other. When his group worked on an obstetric tool in Ghana, they brought in community and religious leaders, whose concern was that revealing fetal sex could encourage sex-selective abortion.
Sensing the body
Professor Sandra Dudley of London South Bank University and Director of the REACT Innovation Centre, described wireless networks moving from carrying data to sensing with it, an approach known as integrated sensing and communication. Edge nodes become local points of sensing and inference, with low latency and continuous monitoring that need not send data to the cloud.

Her group’s projects put the idea to work. MammoWave uses microwave breast imaging and returns an AI-assisted result to a clinician within ten minutes. The same method is now being adapted to the brain, to tell haemorrhagic from ischaemic stroke, and that work has been through feasibility trials at Pisa University Hospital on 60 patients, with the results still being evaluated. A third project uses radar to estimate walking speed, cadence, and stride length, each above 92% accuracy. What these have in common is that the sensing runs over the wireless network rather than inside a hospital, so a result is only as good as the connection that carries it. That, Dudley argued, is where the real difficulty lies. Building a clever device is the easy part. Making it work reliably in everyday conditions, and reach patients equally, is not, and decisions on spectrum, network design, and security will decide whether a rural patient gets the same service as an urban one.
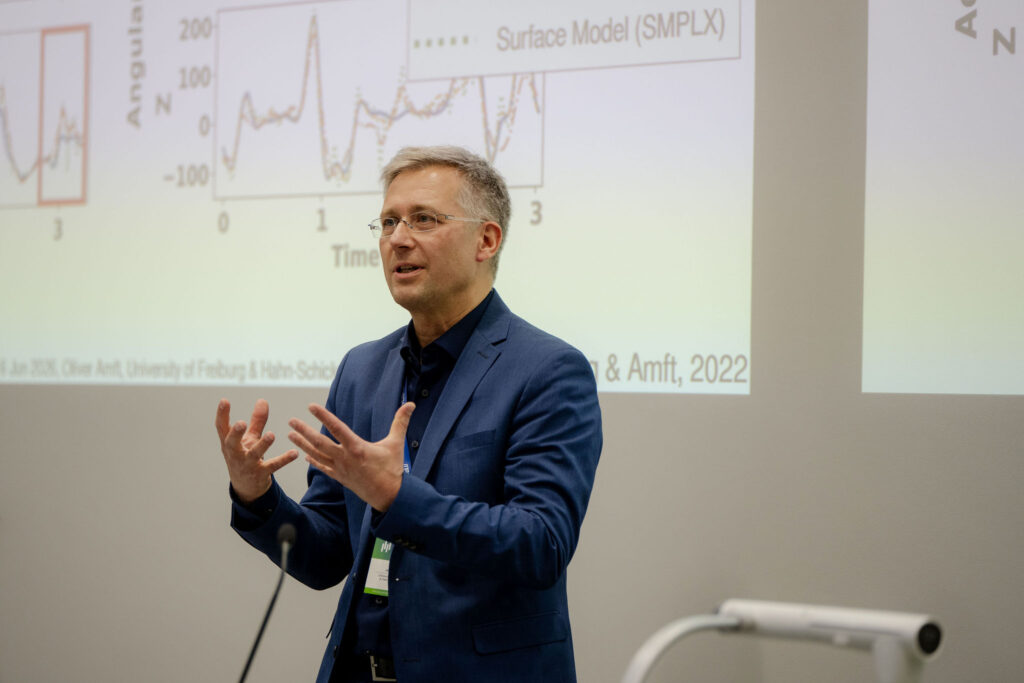
Professor Oliver Amft of the University of Freiburg argued for a shift from pure measurement to co-simulation, pairing a model of the body with a model of the device so researchers can test in a virtual twin where a sensor should sit and what it can detect. Placement matters enormously, and for some gait measurements the error ranges from negligible to as much as 40 to 50% depending on where the sensor is mounted.
His group generates synthetic movement using language and diffusion models, fits virtual sensors and trains on the result, reaching around 80% recognition on fully synthetic data against roughly 90% on real data. He carried the method into optical measurement, and there raised an equity point of his own. Skin melanin strongly affects photoplethysmography, so a sensor that performs well on light skin can read poorly on dark skin unless it is designed not to.
Proving it works

Emmanouil Tsiasiotis of Università Cattolica del Sacro Cuore coordinates EDIHTA, an EU-funded project of 18 partners across 10 countries, finishing in 2027, that is building the first health technology assessment framework designed for digital health. His starting point was that digital technologies evolve in ways drugs and devices do not, so the methods built for those do not fit. EDiHTA is modular, runs across the full life cycle, looks beyond randomised trials, and classifies a technology by its maturity, its intended purpose, and its degree of AI autonomy. Drawn from a review of more than 60,000 papers and combining the Catalan AQuAS model with the EUnetHTA core model, the framework was judged comprehensive at a Brussels workshop in February 2026. The end product is a digital platform with a toolkit, an open-access repository and training materials, with piloting due to begin in September 2026 across nine use cases, three national agencies and six hospitals. Tsiasiotis used the stage to announce that Finland’s HTA coordinating body, FinCCHTA, is joining the consortium and will pilot the framework.
Teaching with new tools

Associate Professor Maryam Alimardani of Vrije Universiteit Amsterdam brought the conference its one talk on education, and a distinct one. Most personalised learning adapts after the fact, once a test or a task has shown how the learner did. Alimardani described learning that adapts in real time, by reading the learner’s brain as they work. Using non-invasive EEG and brain-computer interfaces, her group has trained people in virtual reality and alongside social robots, adjusting the task to the learner’s measured engagement and workload. The worked example came from aviation, where pilots train on a full cockpit simulator. In the MasterMinds project on pilot training, EEG distinguished high from low cognitive workload with 82% accuracy, and feedback tuned to the learner’s brain improved learning over feedback given at random. Her wider point was that the same approach could be carried into how health professionals are trained. Alimardani was equally clear about the limits. Ecological validity, the reliability and accuracy of the interfaces, the lag in adaptation, individual differences and ethics all remain open questions.
What travels and what does not

Associate Professor Smisha Agarwal of Johns Hopkins University gave the closing plenary’s keynote, a comparison across countries. Drawing on the Gates Foundation funded Digital Health Exemplars study, she set out how nations at very different stages digitise primary care, from Rwanda to Finland, and asked what sequence of steps moves a country forward.
Her honest finding was that the gains digital health brings patients lie downstream and are hard to measure, while what is usually visible is efficiency for the system, and only when the work is done well. Brazil’s national primary-care record, Prontuário Eletrônico do Cidadão (PEC), illustrated the argument. Government-built with a public university, it was adopted not by mandate but through financing tied to data-sharing, and, unusually, taken up more readily by poorer and more rural municipalities than by richer ones. A private provider then used the resulting data to target cervical-cancer screening by message, lifting uptake several-fold. Finland’s MyKanta, by contrast, showed no statistically significant gain, which Agarwal attributed to a system already mature and interoperable, with low baseline prevalence. On her summary slide, she put the lesson plainly: ”Equity and sustainability are design choices, not outcomes.” She ended on AI. ”Whenever there is innovation,” she said, ”our hope is much greater than our pragmatism,” so the work has to start with the problem and the population it is meant to serve.

In his closing words, Professor Simo Saarakkala traced the arc the two days had drawn, from Catalonia at the start to Johns Hopkins, Taiwan, and North Ostrobothnia. ”Behind each model there is a patient,” he reminded the room. ”Behind each data set, a citizen who trusted us with something private. Behind each algorithm and implementation study, there is a clinician or nurse trying to do better work tomorrow than today.” His parting instruction was simpler still. ”Take good care of the data,” he said, ”because in the end, it is the people we are taking care of.”
Awards

The conference also recognised its strongest submissions. The awards were chaired by Adjunct Professor Mariella Särestöniemi, of the organising committee, who also presented her own research over the two days. Several of the winning entries returned to themes the invited speakers had raised, from synthetic data and digital twins to the daily experience of staff working with new systems.
Best abstracts
- Aino-Lotta Ilona Alahäivälä, Tunc Asuroglu, Juha Pajula, Ileana Montoya Perez, Tapio Pahikkala and Antti Airola, ”Toward Standardized Evaluation of Synthetic Health Data Across Modalities for the European Health Data Space”
- Raquel Simões de Almeida, Vítor Simões-Silva and Maria João Trigueiro, ”Industry-Driven Project-Based Learning in Digital Health Education”
- Jarmo Mikkola, ”Mechanisms and Conditions for Digital Twin-Enabled Value Co-Creation in Public Healthcare”
Best short papers
- Desmond Hedderson, Helen Monkman, Ian E. Blanchard and Karen L. Courtney, ”Paramedicine Speech Recognition Adoption: A Socio-Technical Ranking Study”
- Thanatcha Satitchantrakul, Niklas Takanen and Ping Jack Soh, ”Liquid-Based Polarization-Reconfigurable Antenna Using Gravitational Method for WBAN Applications”
Best full papers
- Essi Miettinen, Anu Vehkamäki and Märt Vesinurm, ”Extending Customer Journey Modelling Language for Complex Healthcare: A Design Science Research Approach in Kidney Cancer Care”
- Shuhao Que, Dieuwke van Dartel, Ilse Heeringa, Han Hegeman, Miriam Vollenbroek-Hutten and Ying Wang, ”Synthetic Data-Guided Feature Selection for Robust Activity Recognition in Older Adults”
- Egne Annala, Taina Pellikka, Hilkka Korpi, Janna Nadav, Anu Kaihlanen, Paulus Torkki and Elina Laukka, ”Nurses’ Experiences Regarding the Impact of the Implementation of Digital Health and Social Center on Their Work and Other Practices: A Qualitative Interview Study”
Best posters
- Wendakoon Mudiyanselage Kavishwa Bhashitha and Nirnaya Tripathi, ”Self-Adaptive AI in Clinical Decision Support: A Systematic Review”
- Syifaul Fuada, ”Analysis of Available Optical Power in an in-Body Optical Link at 810 nm for OWPT Across Biological Tissue”
Best reviewer
- Chaïmaâ Kissi
Exhibitors
Organisations exhibiting over the two days included Digital Health Finland, OYSTER Incubator, Philips, PLM Group, Polar, TCCF, Esko Systems, Gofore and Nucu. The full list is at nordic-digihealth.com/exhibitors.













Proceedings

The full proceedings are available at nordic-digihealth.com/proceedings.
Browse through the event gallery Browse all the photos from the two days at nordic-digihealth.com/gallery-2026